Do you have a disclaimer?
This question is not frequently asked, but recent polls demonstrate common concerns among the public:
-Optimal treatment depends not just on having the correct diagnosis, but also on understanding each individual patient’s needs and expectations, and their unique circumstances. Treatment in our office is completely individualized, and may vary from person to person for the same diagnosis. Results may also vary from person to person, and are not possible to guarantee. Surgery is not offered unless the expected benefits far outweigh the accepted risks. Surgery is inherently risky, and should be avoided if possible; it is often the last alternative.
-We have no financial interest, or any other conflict of interest, in any health care facility, surgery center, radiology facility, MRI, physical therapy, hand therapy, medical equipment manufacturer, pharmaceutical company, or web link. This office does not solicit or accept gifts or any other inducements from any vendor, and this office does not pay marketing fees. We do not direct satisfied patients to internet physician rating sites. Dr. Ericson has provided consulting services with regard to product design, ergonomics, and expert witness testimony but has no financial interest in any product or service, other than surgery.
What is your cancellation policy?
We are experiencing high demand for services and often have a waiting list for surgical dates as well as office visits. Less than 24 hour notice for a cancellation may result in an administrative fee of $50. Patients who consistently miss appointments without calling to cancel will need to seek care elsewhere.
What should I do with unused post-operative pain medication?
Help protect the environment by taking it here.
I have hypermobile joints that are causing medical problems. Can you help?
Probably. A very useful resource written by Brad Tinkle MD, PhD, a geneticist, can be obtained here. Another resource is the www.chronicpainpartners.com website. As a result of his extensive experience, Dr. Ericson was invited to co-author a journal article on the orthopedic management of the Ehlers Danlos Syndromes, which is available here. Dr. Ericson has given talks at various medical meetings locally, nationally and internationally about this pattern of problems. Also, see the Downloads section of this website. A newer, more comprehensive text is available here.
Have you heard of a newer, safer table saw?
Table saw injuries occur every 9 minutes and are typically unforgiving. SawStop table saws are not new but detect contact with skin and stop blade motion in <0.005 second. This can result in a small finger laceration instead of an amputation.
My private health insurance carrier won’t pay my medical bills. What should I do?
Contact the Washington State Office of the Insurance Commissioner for advice or to file a formal complaint.
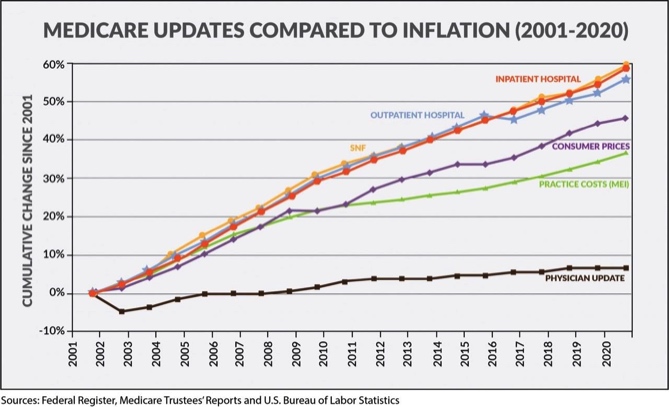
What about Medicare?
Medicare payment rates to physicians have decreased over the past fifteen years, while medical practice costs have steadily climbed. Medicare has also made further arbitrary cuts in reimbursement for specific services provided by physicians, such as total joint replacement surgery, echocardiograms, and electrodiagnostic studies of nerves. These cuts are driving many physicians into hospital employment or out of patient care. Further cuts in physician payment are expected under the guise of reducing the federal deficit; somehow the hospitals have been able to avoid these cuts-
If I have an operation, who does the actual surgery?
Our doctors perform the actual surgery; there are no students, interns, residents, Physician Assistants (PAs), other physicians, or “physician extenders” involved directly in your extremity care, in the operating room or in the office. We do have occasional visitors, with the patient's permission, for observation and education only. After surgery, you will continue to be followed directly your surgeon, not a "physician extender."
If I have surgery, what type of anesthesia will be used?
That depends on a number of factors, including the type of surgery being performed, the expected length of time for the procedure(s), the general health of the patient, and individual preference. With local, regional, and general anesthesia, there are specific advantages and disadvantages to each technique. Please discuss this issue with your surgeon as well as the anesthesiologist.
Do you perform “minimally invasive” surgery?
Yes. We routinely perform endoscopic carpal tunnel release, wrist arthroscopy, needle aponeurotomy and other minimally invasive procedures, when medically appropriate.
If I have surgery, what will the scar look like?
Ask your doctor. Most incisions are closed with absorbable internal sutures that do not need to be removed. The following are typical scars for common operations:
What else about Medicare?
The bureaucracy is stifling. Doctors are responsible for diagnosing and treating patients; getting paid for this is another matter. Consider the following directions on how to bill Medicare for these Evaluation and Management (E&M) Services (this is not a joke):
“Medicare Global Surgery Rules define the rules for reporting evaluation and management (E&M) services with procedures covered by these rules. This section summarizes some of the rules. All procedures on the Medicare Physician Fee Schedule are assigned a global period of 000, 010, 090, XXX, YYY, ZZZ, or MMM. The global concept does not apply to XXX procedures. The global period for YYY procedures is defined by the Carrier (A/B MACs processing practitioner service claims). All procedures with a global period of ZZZ are related to another procedure, and the applicable global period for the ZZZ code is determined by the related procedure. Procedures with a global period of MMM are maternity procedures.
Since NCCI edits are applied to same day services by the same provider to the same beneficiary, certain Global Surgery Rules are applicable to NCCI. An E&M service is separately reportable on the same date of service as a procedure with a global period of 000, 010, or 090 under limited circumstances. If a procedure has a global period of 090 days, it is defined as a major surgical procedure. If an E&M is performed on the same date of service as a major surgical procedure for the purpose of deciding whether to perform this surgical procedure, the E&M service is separately reportable with modifier 57. Other preoperative E&M services on the same date of service as a major surgical procedure are included in the global payment for the procedure and are not separately reportable. NCCI does not contain edits based on this rule because Medicare Carriers (A/B MACs processing practitioner service claims) have separate edits.
If a procedure has a global period of 000 or 010 days, it is defined as a minor surgical procedure. E&M services on the same date of service as the minor surgical procedure are included in the payment for the procedure. The decision to perform a minor surgical procedure is included in the payment for the minor surgical procedure and should not be reported separately as an E&M service. However, a significant and separately identifiable E&M service unrelated to the decision to perform the minor surgical procedure is separately reportable with modifier 25. The E&M service and minor surgical procedure do not require different diagnoses. If a minor surgical procedure is performed on a new patient, the same rules for reporting E&M services apply. The fact that the patient is “new” to the provider is not sufficient alone to justify reporting an E&M service on the same date of service as a minor surgical procedure. NCCI does contain some edits based on these principles, but the Medicare Carriers (A/B MACs processing practitioner service claims) have separate edits. Neither the NCCI nor Carriers (A/B MACs processing practitioner service claims) have all possible edits based on these principles.
Example: If a physician determines that a new patient with head trauma requires sutures, confirms the allergy and immunization status, obtains informed consent, and performs the repair, an E&M service is not separately reportable. However, if the physician also performs a medically reasonable and necessary full neurological examination, an E&M service may be separately reportable.
For major and minor surgical procedures, postoperative E&M services related to recovery from the surgical procedure during the postoperative period are included in the global surgical package as are E&M services related to complications of the surgery that do not require additional trips to the operating room. Postoperative visits unrelated to the diagnosis for which the surgical procedure was performed unless related to a complication of surgery may be reported separately on the same day as a surgical procedure with modifier 24 (“Unrelated Evaluation and Management Service by the Same Physician or Other Qualified Health Care Professional During a Postoperative Period”).
Procedures with a global surgery indicator of “XXX” are not covered by these rules. Many of these “XXX” procedures are performed by physicians and have inherent pre-procedure, intra-procedure, and post-procedure work usually performed each time the procedure is completed. This work should never be reported as a separate E&M code. Other “XXX” procedures are not usually performed by a physician and have no physician work relative value units associated with them. A physician should never report a separate E&M code with these procedures for the supervision of others performing the procedure or for the interpretation of the procedure. With most “XXX” procedures, the physician may, however, perform a significant and separately identifiable E&M service on the same date of service which may be reported by appending modifier 25 to the E&M code. This E&M service may be related to the same diagnosis necessitating performance of the “XXX” procedure but cannot include any work inherent in the “XXX” procedure, supervision of others performing the “XXX” procedure, or time for interpreting the result of the “XXX” procedure. Appending modifier 25 to a significant, separately identifiable E&M service when performed on the same date of service as an “XXX” procedure is correct coding.
What else about Medicare?
Before 2014, if a patient with a simple ankle sprain was evaluated by a physician, the physician would bill the insurer for the office visit using one of the following four ICD-9 diagnosis codes:
845.00 Sprain and strain of ankle unspecified site
845.01 Sprain and strain of ankle, Deltoid ligament/ Internal collateral ligament
845.02 Sprain and strain of ankle, Calcaneofibular (ligament)
845.03 Sprain and strain of ankle, Tibiofibular (ligament) distal
As of 2014, physicians are instead required by the federal government to use one of the following SIXTY ICD-10 diagnosis codes. Wouldn’t the time spent attempting to figure out the correct billing code be better spent helping the patient?
S93.401A Sprain of unspecified ligament of right ankle – initial encounter
S93.401D Sprain of unspecified ligament of right ankle – subsequent encounter
S93.401S Sprain of unspecified ligament of right ankle – sequel
S93.402A Sprain of unspecified ligament of left ankle – initial encounter
S93.402D Sprain of unspecified ligament of left ankle – subsequent encounter
S93.402S Sprain of unspecified ligament of left ankle – sequel
S93.409A Sprain of unspecified ligament of unspecified ankle – initial encounter
S93.409D Sprain of unspecified ligament of unspecified ankle - subsequent enc.
S93.409S Sprain of unspecified ligament of unspecified ankle – sequel
S93.412A Sprain of calcaneofibular ligament of left ankle – initial encounter
S93.412D Sprain of calcaneofibular ligament of left ankle – subsequent enc.
S93.412S Sprain of calcaneofibular ligament of left ankle – sequela
S93.419A Sprain of calcaneofibular ligament of unspecified ankle – initial enc.
S93.419D Sprain of calcaneofibular ligament of unspecified ankle – subsequent
S93.419S Sprain of calcaneofibular ligament of unspecified ankle
S93.431A Sprain of tibiofibular ligament of right ankle – initial encounter
S93.431D Sprain of tibiofibular ligament of right ankle – subsequent encounter
S93.431S Sprain of tibiofibular ligament of right ankle – sequela
S93.432A Sprain of tibiofibular ligament of left ankle – initial encounter
S93.432D Sprain of tibiofibular ligament of left ankle – subsequent encounter
S93.432S Sprain of tibiofibular ligament of left ankle – sequela
S93.439A Sprain of tibiofibular ligament of unspecified ankle – initial encounter
S93.439D Sprain of tibiofibular ligament of unspecified ankle – subsequent enc.
S93.439S Sprain of tibiofibular ligament of unspecified ankle – sequela
S93.491A Sprain other ligament of right ankle (Internal collateral/ talofibular) initial encounter
S93.491D Sprain of other ligament of right ankle (Internal collateral/ talofibular) subsequent encounter
S93.491S Sprain of other ligament of right ankle (Internal collateral/ talofibular) sequel
S93.492A Sprain of other ligament of left ankle, initial encounter
S93.492D Sprain of other ligament of left ankle subsequent encounter
S93.492S Sprain of other ligament of left ankle sequel
S93.499A Sprain of other ligament of unspecified ankle initial encounter
S93.499D Sprain of other ligament of unspecified ankle subs encounter
S93.499S Sprain of other ligament of unspecified ankle (Internal collateral/talofibular) sequela
S93.211A Strain of intrinsic muscle and tendon at right ankle and foot level initial encounter
S96.211D Strain of intrinsic muscle and tendon at right ankle and foot level subsequent encounter
S96.211S Strain of intrinsic muscle and tendon at right ankle and foot level sequela
S96.212A Strain of intrinsic muscle and tendon at left ankle and foot level initial encounter
S96.212D Strain of intrinsic muscle and tendon at left ankle and foot level subsequent encounter
S96.212S Strain of intrinsic muscle and tendon at left ankle and foot level sequela
S96.219A Strain of intrinsic muscle and tendon at ankle and foot level, unspecified side initial encounter
S96.219D Strain of intrinsic muscle and tendon at ankle and foot level, unspecified side subs encounter
S96.219S Strain of intrinsic muscle and tendon at ankle and foot level, unspecified side
S96.811A Strain of other muscles and tendons at right ankle and foot level initial encounter
S96.811D Strain of other muscles and tendons at right ankle and foot level subsequent encounter
S96.811S Strain of other muscles and tendons at right ankle and foot level sequela
S96.812A Strain of other muscles and tendons at left ankle and foot level initial encounter
S96.812D Strain of other muscles and tendons at left ankle and foot level subsequent encounter
S96.812S Strain of other muscles and tendons at left ankle and foot level sequel
S96.819A Strain of other muscles and tendons at ankle and foot level, unspecified side initial encounter
S96.819D Strain of other muscles and tendons at ankle and foot level, unspecified side subs encounter
S96.819S Strain of other muscles and tendons at ankle and foot level, unspecified side sequel
S96.911A Strain of unspecified muscle and tendon at right ankle and foot level initial encounter
S96.911D Strain of unspecified muscle and tendon at right ankle and foot level subs encounter
S96.911S Strain of unspecified muscle and tendon at right ankle and foot level sequel
S96.912A Strain of unspecified muscle and tendon at left ankle and foot level initial encounter
S96.912D Strain of unspecified muscle and tendon at left ankle and foot level subs encounter
S96.912S Strain of unspecified muscle and tendon at left ankle and foot level sequela
S96.919A Strain of unspecified muscle and tendon at ankle and foot level, unspec. side initial encounter
S96.919D Strain of unspecified muscle and tendon at ankle and foot level, unspec. side subs encounter
S96.919S Strain of unspecified muscle and tendon at ankle and foot level, unspec. side sequela
If these issues concern you, please contact your elected Congressional representative:
Contact your US Representative
Or, consider joining the AMA Patient's Action Network.
Who did your website?
Dr. Ericson- ask him about it! It is written in EverWeb, which cost him about $100, plus his time, and then monthly hosting fees.
Click HERE for our Patient Portal
Where is your Patient Portal?
Click here.
Do you take my insurance?
We are currently contracted providers for Blue Cross Blue Shield, FirstChoice, LifeWise, Premera, Regence, and Uniform. We are “Out-Of-Network” for most other carriers and are not contracted with Medicare or Medicaid. Please check with your benefits administrator or your health insurance carrier regarding the specifics of your policy.
Do you treat children?
Generally, no, unless the child has an adult-type problem, or is referred by another orthopedic surgeon or hand surgeon. Please call for additional information.
What should I bring with me to the appointment?
Please bring your insurance information, a picture ID, any previous medical records, radiographs (plain films or CD/DVD), MRIs, EMG/NCVs, operative notes, consultations and anything else you feel might be relevant to your situation. There is complimentary WiFi internet access in the office. If your doctor is running late, we will try to inform you ahead of time; appointments may be delayed by emergencies, coordination of care, required administrative tasks, complicated patients with lengthy medical records, internet and software glitches, and other unanticipated and/or unavoidable circumstances. We apologize in advance, and appreciate your patience!
Do you have any advice as to how to talk to your doctor?
Click here for a helpful podcast from NPR about how to talk to your doctor.
What about Covid?
COVID19 is a highly contagious, potentially fatal viral illness, that is easily spread via air and touch; and, people can be contagious without symptoms. Telemedicine visits are utilized when clinically appropriate. Currently, patients and employees are screened for COVID symptoms, and history of exposure or fever. Patients and physicians wash their hands prior to any physical contact. UV HEPA air filters are in each exam room. State, federal and hospital COVID guidelines change frequently - please inquire about our current protocols.
What about patients traveling from out-of-town?
Please call the office for current information related to Covid and travel. We suggest travel insurance, and recommend obtaining a Covid test prior to traveling.
What about workmen’s compensation claims?
Dr. Ericson is not contracted with L&I. Dr. Oseto is contracted with L&I, but has limited involvement. Please note this office does not open claims, re-open claims, add-on to claims, file appeals, or manage chronic disability. Please call for more details.
What about Independent Medical Exams or liability cases?
Please have your legal representative contact the office directly.
I want to see you, but you are not in my health insurance network, and I have no out-of-network benefits. What can I do?
Seattle is fortunate to have a large number of particularly well-trained orthopedic hand surgeons. You can search for a highly qualified board certified orthopedic hand surgeon through the American Society for Surgery of the Hand, and/or through the American Academy of Orthopaedic Surgeons websites.
“I need some forms signed by the doctor...”
Please submit the forms to the front desk on arrival, at least 72 hours before you need them to be completed; prepayment of a nominal fee is required for some forms. Also, please note that some forms require only confirmation of medical facts and a signature, but others are complicated and can take substantially more time to complete. There is a charge for this service.
Where do Drs. Ericson and Oseto perform surgery
Surgery is performed at the EvergreenHealth Surgery Center in Kirkland, WA, or at the Edmonds Center for Outpatient Surgery in Edmonds, WA.




Resection Arthroplasty



Ligament Repair
Most extremity surgery is done on an ‘outpatient’ basis, meaning that patients come from home on the day of surgery, and are discharged to home following the procedure. Someone must drive the patient home, and the patient must also be discharged to the care of a responsible adult. Generally, this includes patients undergoing “in-office” procedures such as needle aponeurotomy.